

Introduction
Over the past 40 years, therapy intensification has continuously contributed to an improvement in the prognosis of children with AML. Hence, the AML-BFM 2004 trial resulted in a 5-year overall survival rate (OS) of 70%. Similar outcomes backing this claim were obtained by other study groups. During the prospective, randomized AML-BFM 2012 trial, purine analogue clofarabine (C) was introduced to the therapy regimen. Prev. synergistic effects of C combined with cytarabine (A) have been observed in relapsed/refractory ped. AML. It was meant to further increase the antileukemic efficacy in the 1st induction of de novo AML. Clofarabine (C), liposomal daunorubicin (Dx; L-DNR), and cytarabine (A) were randomized against to the stand. induction course of cytarabine, etoposide (E), and L-DNR. The implementation of a stand. stem cell transplantation (SCT) indication for patients with HR AML was another progress. The trials' primary obj. was the improvement of event-free survival (EFS) in ped. AML.
Patients and Methods
AML-BFM 2012 was an open, interventional, multi-center, prospective, randomized clinical trial for patients with de-novo childhood AML (age<18 years), comparing the use of clofarabine (CDxA) and etoposide (ADxE) in the 1st induction course. Recruitment began in 02/15. Since 11/17 the auxiliary drug, L-DNR, was no longer commercially available. With the use of CDxA being discontinued, this resulted in both the CDxA and ADxE arm being replaced with the alternative stand. arm, AIE. Upon permanent unavailability of the L-DNR, the study was terminated early. The total no. of recruited patients was 164, instead of the initially planned n=500.
Results
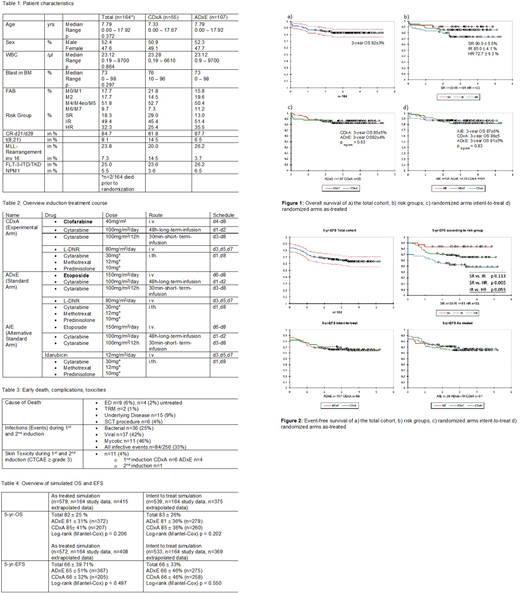
With a 3-yr OS of 82 ± 3% & 3-yr EFS of 69 ± 4%, respectively, children treated by AML-BFM 2012 have an excellent outcome (median FU: 3.03 yrs.), which is superior to previous trials. The outcome did not significantly differ between ADxE and CDxA. In the study n=9 early deaths (EDs; defined as death <d42) were observed, in n=4 no treatment was initiated before the death. N=2 died from treatment-related mortality (TRM; 1,2%) in CR; in another 6 patient's death was assoc. with toxicities or complications from allogeneic SCT (3,7%). Severe infections were the most common complications; 32.8% of all reported infections were observed during the 1st or 2nd course. Prompted by the skin toxicity levels relating to C found in lit., upon closer observation, 11 events in total were categorized to the CTCAE grade ≥3 in both the 1st & 2nd cycle. 6/11 events were assoc. with C.
Two statistical simulations were used to determine the potential significance of the study's primary obj., if 500 patients had been enrolled. In both simulations, the same progress was assumed for the patient outcome, only extrapolated to the required no. of cases. In the 1st simulation, the actual randomization compliance was retained in favor of the stand. arm ("as treated" simulation). In the 2nd calculation, therapy groups were weighted according to the planned intent-to-treat ratio of 1:1 ("intent to treat" simulation). Various simulated case nos. were translated into whole nos. to fulfill the criteria for the Kaplan-Meier analysis. Neither calculation shows a major effect on EFS or OS for either arm.
Conclusion
The treatment regimen used in AML-BFM 2012 has an excellent overall outcome, which exceeded outcomes from previous trials. The outcome is not only a result of the intro. of C, despite its potential effectivity in ped. AML. The results are closely linked to a better risk group stratification, improvements of allogeneic SCT in HR patients, and better supportive care. Since L-DNR was successfully evaluated in ped. AML in first and second-line treatment (AML-BFM Study 2004 (Creutzig et al. 2013) / Int. Relapsed AML 2001/01 (Kaspers et al. 2013)), incl. a possible reduction of anthracycline-induced cardiomyopathies, the unavailability of L-DNR due to industrial reasons resulted in severe damage in the treatment devel. in children with malignancies. More early clinical trials are vital to further examine other neoadjuvant drug combs. that replace L-DNR.
In summary, AML-BFM 2012 showed an improvement of EFS and OS. Forced termination of clinical trials for commercial reasons is ethically dubious. Pharmaceutical companies need to act responsibly regarding clinical trials involving sick children. The introduction of C as the first-line treatment of ped. AML should be considered feasible.
Reinhardt:Janssen: Membership on an entity's Board of Directors or advisory committees; Celgene Corporation: Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Membership on an entity's Board of Directors or advisory committees; CLS Behring: Research Funding; bluebird bio: Membership on an entity's Board of Directors or advisory committees; Roche: Research Funding.
Clofarabine, Etoposide, liposomal Daunorubicine using in AML frontline treatment in children

